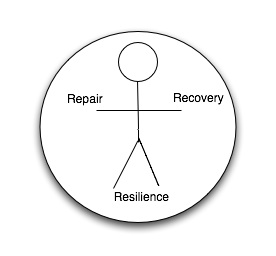
Here’s a diagram I drew last night.
This works for me as a symbol of what health care should do.
In the middle we see the symbolic representation of a person. All health care should be focussed on the individual. It’s this person with me today who needs my attention. It’s this person in their uniqueness who needs to be understood and cared for. It’s the whole of this person who is with me today (not just the bit of them that’s not working!)
There are three Rs –
- Repair
- Recovery
- Resilience
Most treatments are directed at repair. Dilating constricted airways, reversing spasm of arteries, killing infecting organisms etc. But we only become well again by recovering from an illness. If we have an infection then an appropriate antibiotic might kill the bacteriae but it’s our body’s processes of healing and recovering which restore our tissues and our whole beings to health. The processes of recovery are not so well understood and very few medical interventions claim to stimulate or enhance recovery, but we see reports like this which show that the patients’ emotional state influences recovery for example and some research has shown that the physical environment in which a patient is nursed influences recovery. In other words, recovery is not about just dealing with the disease, recovery is about addressing the whole person in the context of their environments.
Finally, after recovery, can we do anything to reduce the chances of this person falling ill this way again? Can we increase their resilience? So much of preventitive health these days is a technical fix – drugs – drugs to lower blood pressure and cholesterol for example – but the best way to be healthy and to stay healthy is to be more resilient – and that involves not just the physical body but the whole person in the context of their life. Not so much is understood about resilience and very, very little exists in health care to specifically address and enhance an individual’s resilience.
Wasn’t it Benjamin Franklin who said
God heals and the doctor takes the fees
Well, that’s not good enough any more. We need more research to understand the processes of recovery and resilience and we need to ask the question of health care – how does this intervention address the patient’s needs for Repair, Recovery AND Resilience? And if the intervention ONLY addresses repair, then what else are we going to do to address both Recovery and Resilience? Because without addressing these needs we are fighting a continually losing battle of repeated repairs.
When the NHS was created in the UK, the Labour government genuinely believed that providing health care for all would so improve the health of the nation that the costs of the service would fall year by year. It never happened. Quite the reverse. Why? Because they created a National Repair Service, not a National Health Service. (well, that’s part of the reason, another part is that health is a much more complex phenomenon than can be addressed by a health care service – poverty, housing, sanitation, education and work and so on are HUGE influences on health experience too)
There’s one final element to this little drawing. The circle around the person. This represents understanding that we need to address a whole individual within the context of their life, and also represents that a person needs cared for by a circle of carers. Health including recovery and resilience is influenced by that complex network of individuals – professionals, friends and relatives who surround the person.
Fundamentally, though, the circle represents CARE – nobody really gets better unless someone cares for them. All health care should be delivered by people who CARE.
Read Full Post »