
I was reading an interview with Harvard historian, Anne Harrington, who has written “Mind Fixers: Psychiatry’s Troubled Search for the Biology of Mental Illness”.
When I was at university I was taught there were two types of depression – reactive and endogenous – the former occurring in response to specific events, and the latter seen as an illness of internal origin. It was thought that talking therapies, as they’ve come to be called, were the best way of dealing with reactive depression but that endogenous was a biological problem which required drugs. One of the main themes which emerged from that thinking was the serotonin theory of depression which was the basis for the great commercial success of Prozac, a drug which influenced the levels of serotonin in the brain.
Well, it all changed. Psychiatrists stopped distinguishing between “reactive” and “endogenous” and moved to thinking of all depression as biological and, hence, all requiring treatment with drugs.
But that didn’t last. As Anne Harrington describes, in the late 90s, “a range of of different studies increasingly seemed to suggest that these antidepressants – although they’re helping a lot of people – when compared to placebo versions of themselves, don’t seem to do much better.” As the “gold standard” of drug effect is its performance over that of placebo, and drug after drug was shown not to be that much better, it got harder and harder to bring new drugs onto the market. She says –
“But it doesn’t mean that the drugs don’t work. It just means that the placebo effect is really strong. But the logic of clinical trials is that the placebo effect is nothing, and you have to be able to better than nothing. But of course if the placebo effect isn’t just nothing, then maybe you need to rethink what it means to test a drug”
This is the same observation as Irving Kirsch made in his “Emperor’s New Drugs”. In that book he drew a graph which I found very impressive –
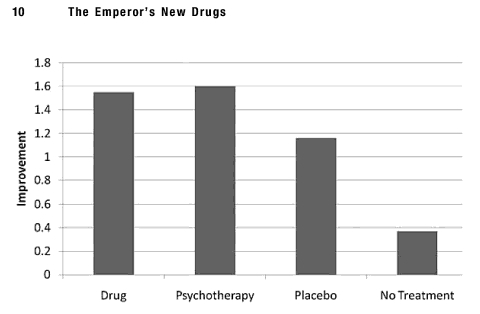
The point he was at pains to make was the same as Anne Harrington’s – well, actually, he was trying to emphasise that just because the drugs didn’t seem much more effective than placebo didn’t mean that doctors should stop prescribing them. But the main point, I think, is –
Placebo is not nothing
It seems crazy to me that people make decisions about whether or not a treatment should be offered to patients solely on the basis of its statistical difference to placebo if those decisions then lead to the withdrawal of treatments which were helping thousands of patients.
If the placebo effect is not the same as doing nothing (and it is clear that it is NOT the equivalent of doing nothing) then we should be exploring just what it is. That will involve moving on from the stigma of trickery, because that’s how the placebo effect has been portrayed. “Dummy pills”, “inactive pills”, “mock treatments” producing real life changes in the patients who receive them, only to reveal to them that, ha! ha! you got nothing!
I think it’s interesting that it is in the area of psychiatry that this debate has emerged. Because we know something of the power of placebo on our mental states. But as we are whole, body/mind, non-dual beings. What influences our mental states, influences our bodily functions too. Placebo effects are not restricted to changes in mental states, they are seen throughout the body, influencing organs, cells and circulating levels of natural chemicals.
Here’s the other thing – if placebo is NOT the same as doing nothing but a drug doesn’t show a substantial and significant benefit over placebo, then what else can we offer the patient? What else will be at least as powerful as placebo, but less harmful than the drug?
What about exercise, nutrition, the creation of significant social relationships, engagement with natural environments, meditation, learning how to handle our emotions for starters? And not forgetting demanding that we do something about the conditions in which more and more chronic illnesses are emerging – both mental and physical – poverty, poor housing, inequality, polluted environments, industrial, chemical methods of agriculture and food production and so on – have a look at the perspective I described in “There still aren’t enough”, and in “Inequality and health”.


Leave a comment