There is a big difference between what is complicated and what is complex.
A machine can be very complicated. As cars have become ever more sophisticated they have become more complicated. It’s not easy to see what’s wrong when your car breaks down, unless you have learned how it works.
Machines are made up of different parts, and there may be hundreds or thousands of parts in a machine but we can still learn exactly how it works and how to fix it by learning bit by bit just how each part works and how it affects any other part.
People on the other hand are complex. We also are made up of many many parts, billions and billions of cells, each of which is an agent acting on many other cells, and each of which, in turn is acted upon by many other cells. In fact, through the multiplicity of interactive connections which exist, it becomes impossible to deal with any single part in isolation, or, indeed, to be able to accurately predict the over all effects of any single change. It’s parts don’t necessarily function the same way in isolation as they do when under the influence of their multiple connections.
This structure makes the organism a complex one, not a complicated one.
Here is the key difference –
A complicated structure can be understood by understanding its individual parts.
A complex one can only be understood as a whole.
Archive for the ‘health’ Category
Complicated or complex….what’s the difference?
Posted in from the consulting room, health, science on February 13, 2013| Leave a Comment »
Health is an experience. Can we agree about that?
Posted in from the consulting room, health on February 7, 2013| Leave a Comment »
Health is not a THING.
Health is not an entity or a product.
Health is more than the sum of the set of “normal” measurements.
Health is a lived experience.
As an experience, health is a characteristic described by the experiencing person, by the subject. Without a person to experience health, there is no health.
So, why do we deliver health care by treating diseases and people as objects, or by processing people to reach pre-determined targets, which might have precious little to do with the experience of health?
The shocking report on Stafford Hospital, suggesting between 400 and 1200 patients might have died due to the way they were treated in the hospital concludes that
“There was a lack of care, compassion, humanity and leadership,” he said. “The most basic standards of care were not observed and fundamental rights to dignity were not respected.”
Chris Ham of the Kings fund says
The priority must be to shift from a culture in which the behaviour of staff is driven by compliance with targets to one in which there is a real commitment to patient-centred care in every hospital and surgery
But so far the government’s response seems to be to drive towards greater compliance with tougher regulation and inspections.
The problem isn’t one of control, it’s one of “care, compassion and humanity”. How did the Health Service come to this?
Increasingly we treat health care delivery in the same way we treat a business or a factory, by measuring, standardising, and enforcing compliance. None of that seems to be improving the experience of health care because none of that is based on the fact that health is a lived experience, not a product.
Every single human being is unique.
Every life is unpredictable.
A truly patient-centred care will consider the uniqueness of the individual at all stages in the health care journey, and will require imagination – the imagination needed to enable health care workers and managers to imagine what it would be like to experience what the patients are experiencing.It will also take a lot of non-judgemental listening. Without really hearing a person’s story, we fail to know their uniqueness, fail to comprehend or consider their beliefs, values or wishes.
The Stafford story is not the end of the story. It’s probably the tip of an iceberg. Maybe now is a wake up call for all of health care. Maybe now is the time to reconsider the commodified, reductionist, materialistic basis of the current model which pushes more and more drugs into more and more people every single year, and processes more and more people through hospital beds ever more quickly.
After all, if health is an experience, we should design health care around making personal experiences better.
Check out the manifesto for slow medicine.
Plots and Fate
Posted in from the consulting room, from the living room, health, life, narrative on January 13, 2013| 2 Comments »
Each of us lives out a story, a dynamic narrative whose only consistency is that we somehow show up in each of the scenes. While the plots line may be unknown to us, there is one. Creating a Life. James Hollis
We know ourselves and others through the stories we tell. We create meaning and gain an understanding of the events and experiences of our lives by creating a narrative. And isn’t that quote so true? Doesn’t it sometimes seem as if the only constant in our life story is that we show up in each of the scenes. All of life, the world we live in and experience, is woven into these stories, which always, in some way, contain ourselves.
But what about this idea of a plot? Because doesn’t it happen to all of us that from time to time we lost the plot? In fact, don’t many people never seem to have a grasp of the plot? Well, an interesting factor in the creation of the plot comes from thinking about Fate.
What is fate?
The narrower the frame of consciousness, the greater the personal chronicle plays out as fate…what is denied inwardly, will come to us as Fate. Creating a Life. James Hollis
Of course, we have the hand we are dealt too, as part of Fate. Sir Harry Burns, the Chief Medical Officer of Scotland, in discussing the problems of ill health in Scotland points the discovery that a grandfather’s experience can alter his genes and so pass on influences that way through his children and even their children too. We can’t understand a person, or their plot, without seeing who they are within more than their own personal lifetime. We have to consider their genetic, familial, cultural and societal contexts and influences, most of which may shape the unconscious more than they shape the conscious. Living a zombie life, on automatic pilot, will be experienced as a life dominated by Fate, but waking up, becoming conscious, examining our own lives, gives us the chance to become the heroes of our own personal stories.
Plot is partly unearthed, and partly created.
Conformity overload?
Posted in from the consulting room, from the living room, health, life on January 9, 2013| 1 Comment »
As Howard Bloom points out in The Global Brain, there are a couple of opposite but essential drivers at the heart of complex systems – conformity enforcers and diversity generators.
We need both. But we need both to work together in an integrated way. If there’s too much of either growth, development and evolution is impeded.
Diversity generators don’t just tolerate difference but give highest value to uniqueness. Conformity enforcers, on the other hand, operate by eliminating difference, setting standards and rules and making sure the whole system is compliant.
In health care, it seems to me, we have an excess of conformity enforcement. The “evidence based” enforcers seek to “eliminate variation” by developing flow chart style protocols where every single patient is entered into the same pathway and is treated according to the same, limited range of interventions. There is a belief that the raw material of patients can be entered into the same machine and will come out the other end with the same product or “outcome”.
But life isn’t like that. Every single human being is unique. There isn’t a single health care intervention in the world which produces the same outcome for every patient who receives it. There’s something essentially dehumanising about the enforcement of conformity on the rich diversity of individuals.
I’m a champion for diversity and tolerance. I think it’s richer than uniformity and conformity. I don’t deny that we need some level of conformity (without it we’d have disintegration and chaos), but I think we’ve gone too far. Not just in health care but in many, many areas of modern society – education, politics, economics…….
Where do you put your energies? Are you throwing your weight behind diversity generation or conformity enforcement?
What’s the story?
Posted in from the consulting room, health, narrative on January 8, 2013| 1 Comment »
I saw this cartoon the other day and there was immediately something about it that bothered me….
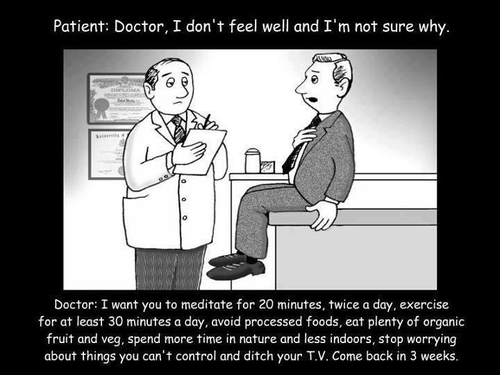
……what was it?
The advice from the doctor….well, I say all of those things. Not exactly as said here, but pretty close. I suspect any doctor giving advice about health probably covers a selection of these points nowadays. Maybe some would talk about “5 a day” instead of “plenty of organic fruit and veg”, and some would mention stopping smoking and drinking in moderation, but it really covers the common advice.
So, what’s the problem?
Well, the problem is you can imagine from this cartoon that this advice has become like a standard prescription. A modern panacea. Doesn’t matter who the person is, or what they are complaining about, here’s the same advice.
Who is this man in the grey suit? When he says he doesn’t feel well, what exactly does he feel? And what really are his concerns? Why has he come to the doctor as this particular point? In other words, who is he, what kind of life does he lead, and how does his illness experience fit into his life story? (There’s a clue that he is seeking a meaning when he says “I’m not sure why”
What’s missing?
The person – because we aren’t hearing the story.
Here’s the text of a post I wrote on this blog four years ago about the importance of story (the importance of story, you’ll see, is a main theme of this blog)
The people who come to see us bring us their stories. They hope they tell them well enough so that we understand the truth of their lives. They hope we know how to interpret their stories correctly. We have to remember that what we hear is their story.
Robert Coles in “The Call of Stories”.
Stories have always fascinated me. I love them. Every day when I sit in my consulting room patients tell me the most amazing, fascinating and unique stories. As a medical student I was taught how to “take a history” – I hate that phrase actually – who’s doing the “taking” and what exactly are they “taking” and from whom? Doesn’t seem right to me at all. Instead I prefer teaching medical students how to listen to patients’ stories. However, the point is that this is the beginning of all diagnosis. To a certain extent listening to the patient’s story is a diminished art. There’s an over-reliance on technology and a lot of doctors just don’t seem to be able to make a diagnosis without a test these days. Diagnosis is a form of understanding. It’s a process of trying to make sense of somebody’s experience.
If stories are so important in clinical practice, then how can I learn to handle them better I wondered? There is a developing area of medicine known as “narrative-based practice”, with associated “narrative-based research” methodologies, but materially-orientated, reductionist scientists look down on narrative. They prefer data. So, when I started to study narrative (which, technically is the story AND the way that story is told), I couldn’t find much work from a scientific perspective. I had to turn to the humanities.
One of the books which I really love in this area of study is “On Stories” by Richard Kearney (ISBN 9-780415-247986). Not only is it a fabulous exploration of the place of story in human life, but it’s written completely beautifully. Richard Kearney is a philosopher but he’s also a magnificent writer. This one book taught me more about the importance of story than any other.
Telling stories is as basic to human beings as eating. More so, in fact, for while food makes us live, stories are what make our lives worth living.
This sets stories at the heart of human existence – not optional, but essential.
Aristotle says in “Poetics” that storytelling is what gives us a shareable world.
The key word there is “shareable”. It’s through the use of story that we communicate our subjective experience and its through the sharing of subjective experience that we connect, and identify with others.
Without this transition from nature to narrative, from time suffered to time enacted and enunciated, it is debatable whether a merely biological life could ever be considered a truly human one.
Beautifully expressed. Sets narrative at the heart of what it means to be human and stands it against those who would take a materialistic view of life which they claim can be reduced to data sets and DNA.
Every life is in search of a narrative. We all seek, willy-nilly, to introduce some kind of concord into the everyday discord.
This is one of my favourite lines in the whole book. This is exactly the power of story – it enables us to “get a handle on” life, to bring some kind of order out of chaos.
What does Richard Kearney mean by story then? Well, I’ll finish this post with two more quotes from his book which make it very clear and very simple.
When someone asks you who you are, you tell your story. That is, you recount your present condition in the light of past memories and future anticipations.
This shows that story collapses time, bringing the past and the future into the present. Story telling requires memory, imagination and expression.
Every story requires –
a teller, a tale, something told about, and a recipient of the tale.
Nice and simple, but what profundity lies in there. For every story, there is a unique human being doing the telling, there is the story itself and its subject matter, and, very importantly there’s the recipient – the listener or the reader. Story is, as Aristotle said, a way of creating a shareable world. That’s the greatest potential of blogs, I reckon. By sharing our stories we create a shared world. Yes, sure, stories can divide as well as connect, but without stories, there is no potential for connection, no potential for compassion and no potential for the creation of a meaning-full, and better world.
Self in relationship
Posted in from the consulting room, from the living room, health, life, personal growth, psychology on January 7, 2013| 3 Comments »
The self is relatedness. The self doesn’t exist without relationship. The self appears in your deeds, and deeds always mean relationship.
James Hollis wrote that. It stopped me. You find there are books like that, don’t you? Books which you can’t read all the way through without stopping. I don’t mean the stopping for tea, or to answer the phone. I mean that stopping in the middle of the page, or anywhere in the page actually, because what you just read provokes such a mental reaction. This was one of the many places where I stopped when reading Creating a Life by James Hollis.
My first thought was, “how true”. I see connections everywhere, and I see the constancy of change. In fact, that is so important to me that I put the phrase, “becoming not being….” as the sub-head of this blog.
We are constantly becoming, ever interacting, exchanging, adapting and changing.
So, it’s true. The self doesn’t exist without relationship. I’ve thought many times that you could never know a person by observing them, through a one way glass,in an empty room. You have to see how a person interacts, with you, or with others, to have any sense of who they are.
Reminds me too, of “Ubuntu” – “I am because you are”
But then it seemed to me he’d gone too far when he added “deeds always mean relationship”.
Surely there must be deeds we commit alone?
But hold on, am I narrowing the definition of relationship too far here? Am I assuming a relationship is between two PEOPLE?
What about how I relate to Nature, to the built environment, to music and images and art? To this very book I am reading in fact!
It’s true what he says – the self really does appear in our actions, our reactions, and our interactions. It’s not a phenomenon which emerges in total isolation (even our memories and our imaginings are the creation of relationships aren’t they?)
So here’s something to consider today – what sense of self do I notice emerging from my deeds? my choices? my interactions?
The suffering gap
Posted in from the consulting room, from the living room, health, life on January 6, 2013| 6 Comments »

I come across this issue all the time – there is a gap between reality and fantasy, and that’s where suffering occurs.
By fantasy, I really mean imagination, but that includes hopes, dreams, and idealised wishes for how things could be. It includes memories too, because I don’t believe memories are like objects tucked into some cerebral drawer – we recreate them, imagine them anew, every time we bring them into the present.
Some terrible things happen to people. Things that will never go away. And those things keep jumping into the present. We wish those memories weren’t there. We wish those things had never happened, those words had never been said, those choices had never been made. But they did and they were. And in that gap, in that space or difference between how we wish things had been and how they actually were, there’s where suffering lies – hurt, pain, anger, sadness, regret…..
Some people imagine how things might turn out, and those imaginings might either be terrible and they live them now in the fears and paralysing anxieties which emerge in the space between the awful future and the actual present. Or they imagine how things would be so much better than they are and in that gap they find frustration, dissatisfaction and discontent.
What do we can we do with this gap? Can we narrow it a bit, even if we can’t make it go away?
Partly. But, wait a minute. Should our first thought be “let’s get rid of this suffering”? Because if it is, we might reach for the painkillers and the sedatives, or hit the escape routes, before we understand what this pain is about. Might it not be better to see if we can see what the roots of this pain are? Where is it coming from? Why is it here? What sense do I make of it? We are meaning seeking creatures and we want to make sense of lives. What sense do we make of this particular suffering? What it is telling us?
Sometimes, when we understand the suffering better, we understand that something needs to change, that we need to make different choices. And sometimes when we understand it better, we realise that right now, right here, in the present moment, we are actually ok. Better than that, we discover that the everyday, so called ordinary world, right here, right now, is extraordinary and amazing, and that our suffering is fear or anxiety about what might be, overwhelming the present moment and hiding from us the fact that life, here and now, is not just welcome, but something to be grateful for.
There’s another role for suffering of course – creative energy. In the gap between how things are and how we imagine they could be, dissatisfaction or discontent can drive creative solutions, generate new ways of thinking or inspirational art. (I’m not saying you have to suffer to create great art – I’m just saying that sometimes great artists turn their alchemical skills to their suffering and their struggles and create gold)
Anyway, however you handle it, whatever choices you make, next time you feel you are suffering…..Mind the Gap – and reflect on why it’s there. Then you might be able to make a different choice.
Attending the soul
Posted in from the consulting room, from the living room, health, life, tagged health, james hollis, mental-health, science on January 5, 2013| 1 Comment »
There’s a chapter in James Hollis, the Jungian analyst’s book, Creating a Life, entitled, “Attending the Soul”. This particular chapter is about the practice of psychiatry and he completely nails an important point.
If we consider health, acute and chronic illness, to be a spectrum of experience, then we need to do more than control or manage disease in order to be healthy.
Here’s how James Hollis puts it….
In seeking scientific verification of success, many of these practitioners [psychiatrists] have narrowed the definitions of pathology to behavioural patterns, faulty cognitions and flawed chemistry. While it is certainly true that we are behaviours, and behaviours may be corrected, and we are cognitions which may be challenged by other cognitions, and we are chemical processes which may be compensated by other chemical processes, none of these modalities – behaviourism, cognitive restructuring and psychopharmacology – should be confused with psychotherapy.
He goes on to say that psychotherapy seeks to address the whole person, even the meaning of the person, the meaning of their suffering or even the meaning of their life.
This same point applies across the whole of Medicine. Illness may include physical pathologies which can, and may, be addressed with drugs or surgery, or it may include adaptive, or protective symptoms and behaviours which can be changed. However, if we are interested in healing, in facilitating the experience of wellbeing, resilience, and health, then we face the fact that a whole human being is more than the sum of his or her parts.
Here’s how he concludes his chapter…
To stop at behavioural change, as important as it is, or cognitive restructuring, liberating as it may be, and pharmacology, necessary as it sometimes becomes, betokens a failure of nerve and sells the soul very short indeed.
The spectrum of health and illness
Posted in from the consulting room, health on January 4, 2013| 1 Comment »
To describe health as the absence of disease is inadequate and unsatisfying. We have defined diseases for the last four hundred years or so according to the presence of certain lesions, or the presence of “abnormal” readings measured by instruments of investigation. Illness is a related, but different, term from disease. It is used mainly to refer to the experience of being unwell, incorporating our concept of disease, but actually describing the subjective experience of a person. Only a person can tell you they feel nauseated, or that they have pain. Instruments won’t reveal those phenomena.
Similarly, health should be understood as a phenomenon, or an experience, in its own right. For sure, if you have either a disease or an illness, this will impact on your experience of health, but is it really such a black and white issue? I don’t think so.
Consider these three concepts as a spectrum

H = health; A = acute disease; C = chronic illness
From the condition of health, we can move rapidly into the red zone as we experience an acute illness. Think of “winter vomiting”, which only this morning was reported as having affected one in every five people in Scotland this winter. Suddenly, you feel unwell, and then you start to vomit, and/or, have diarrhoea. You pretty much have to wait it out, resting, and replacing the fluid losses as best you can. Although caused by a virus, we don’t have antiviral drugs which effectively and quickly kill this particular one (and even if we did, killing the virus is only one part of becoming well). What helps?
The body heals itself. Any intervention, including rest and replacing fluids, will only help by supporting the body’s capacity to self-heal. Personally, I and my family, used homeopathic medicines in addition, to speed our recovery from this nasty acute illness.
In other acute situations, relying on the body’s self-healing is not enough. In the situation of acute heart failure, a heart attack, severe acute asthma, a diabetic crisis (hypo or “DKA”), and so on, medical treatments including drugs or surgical procedures can make the difference between living and dying during this acute event.
However, once the acute episode settles, the person may move up into the healthy blue zone of the spectrum, or may slip around into the chronic yellow one. We see this in diseases such as MS (Multiple sclerosis), where the acute episode might settle completely and the person returns to an experience of health, or it might progress into a more chronic pattern.
Similarly, someone might develop a chronic illness insidiously, without any acute episode at the outset, and they might move towards the healthy zone, or they might occasionally fall directly into the acute red zone as they experience a flare-up (as we might see with inflammatory bowel disease, for example).
Why is this spectrum helpful?
Well I think it shows that health, acute and chronic disease and illness, are different, but related phenomena. However, it also shows us that different tools are required depending on where the person is on the spectrum. There are drugs and operations which can assist in the management of problems in the acute or chronic zones, but any movement towards health always requires the good functioning of the individual’s self-healing capacity.
This is one of the main things I find missing in modern health care. We attend to the lesions and dysfunctions, but we lack the technologies for directly supporting and stimulating the body’s necessary self-healing capacity.
This is the area being explored by doctors interested in “integrative medicine” ie interventions which are intended to support greater integration or coherence of the whole system.
We need research to better understand self-healing. In fact, we need to become better able to describe and understand the condition we call health. If we want to increase the health of populations we will probably find the answers, not in drugs, operations or therapies, but in creating the conditions, and supporting the contexts, for adaptation, creating and engagement – characteristics of health.
In relation to illness, however, we also need to explore interventions which are intended to be integrative by examining their impact on health, not on lesions.
Separate and connected, the heart of opposites
Posted in from the consulting room, from the living room, health, life, personal growth on January 3, 2013| 2 Comments »
For many years when I’ve taught about the different ways in which we develop an identity I’ve described a line with two poles.
At one end is “I”, the unique, separate, different “me”. We have a whole body system, the immune system, developed to be constantly on the alert for what is not “I”, whether it be a virus, another person’s genetic material, or a chemical substance from “outside”. The immune system is primed to quickly recognise any such foreign material and isolate or remove it.
At the other end is “we”, the connected self, the “me” which is part of “we”, whether that be in relationship with another single person, or with a group.
We all need to know that we are unique, that we are different and separate from others. What can come with that however, is a sense of disconnection, or loneliness. Just as importantly we need to know that we are connected, that we belong, that we “fit in” and that we love and are loved. What can come with that can be a loss of personal identity, a feeling of just being a number within the group.
I pointed out that this line with its two poles didn’t have a point somewhere along it where everything was balanced. It doesn’t work like that. We move continuously along the line, back and forth, changing our focus, our awareness and our sense of self, but never wholly living at only one of those poles.
Then last year, I read two books which mentioned concepts which fitted right in to this simple diagram. Thomas Berry’s The Great Work, where he beautifully describes the twin polar opposites of “wildness and discipline“.
When first the solar system gathered itself together with the sun as the center surrounded by the nine fragments of matter shaped into planets, the planets that we observe in the sky each night, these were all composed of the same matter; yet Mars turned into rock so firm that nothing fluid can exist there, and Jupiter remained a fiery mass of gases so fluid that nothing firm can exist there. Only the Earth became a living planet filled with those innumerable forms of geological structure and biological expression that we observe throughout the natural world……….The excess of discipline suppressed the wildness of Mars. The excess of wildness overcame the discipline of Jupiter. Their creativity was lost by an excess of one over the other.
The greater the wildness, the greater the emphasis on “I”, on separateness. The greater the discipline, the greater the emphasis on “we”, on the bonds, the connections.
And Howard Bloom’s The Global Mind, where he picks out five characteristics of complex adaptive systems and highlights the first two as “diversity generators” and “conformity enforcers”. Diversity generators increase the wildness and the sense of “I”, whilst the conformity enforcers increase the discipline and the sense of belonging.
I now have two lists with a line connecting them, and it still didn’t look right. It wasn’t a simple spectrum for example, and it wasn’t a line where there was some balanced point half way along where we “should” be. So, I turned the horizontal line into a vertical line running between the two lists, and then I bent the line into an “S” shape. Drawing a circle right around the whole image turned it into a yin yang symbol and I thought, “Yes, that’s it” – that’s the heart of the universe.

-

This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.5 UK: Scotland License. -
Join 2,089 other subscribers
Top Posts
Categories
- art
- books
- creativity
- education
- from the consulting room
- from the dark room
- from the living room
- from the music room
- from the reading room
- from the viewing room
- health
- humour
- life
- movies
- music
- narrative
- neuroscience
- perception
- personal growth
- philosophy
- photography
- psychology
- science
- Uncategorized
- video
- writing
Pages
Meta
Category cloud
Commenting Policy
Archives
- June 2026
- May 2026
- April 2026
- March 2026
- February 2026
- December 2025
- November 2025
- October 2025
- September 2025
- July 2025
- June 2025
- May 2025
- April 2025
- March 2025
- February 2025
- January 2025
- December 2024
- November 2024
- October 2024
- September 2024
- August 2024
- July 2024
- June 2024
- May 2024
- April 2024
- March 2024
- February 2024
- January 2024
- May 2023
- April 2023
- March 2023
- February 2023
- January 2023
- December 2022
- November 2022
- October 2022
- September 2022
- August 2022
- July 2022
- June 2022
- May 2022
- April 2022
- March 2022
- February 2022
- January 2022
- December 2021
- November 2021
- October 2021
- September 2021
- August 2021
- July 2021
- June 2021
- May 2021
- April 2021
- March 2021
- February 2021
- January 2021
- December 2020
- November 2020
- October 2020
- September 2020
- August 2020
- July 2020
- June 2020
- May 2020
- April 2020
- March 2020
- February 2020
- January 2020
- December 2019
- November 2019
- October 2019
- September 2019
- August 2019
- July 2019
- June 2019
- May 2019
- April 2019
- March 2019
- February 2019
- January 2019
- January 2018
- June 2017
- May 2017
- April 2017
- March 2017
- February 2017
- January 2017
- December 2016
- November 2016
- October 2016
- September 2016
- August 2016
- July 2016
- June 2016
- May 2016
- April 2016
- March 2016
- February 2016
- January 2016
- December 2015
- November 2015
- October 2015
- September 2015
- August 2015
- July 2015
- June 2015
- May 2015
- April 2015
- March 2015
- February 2015
- January 2015
- December 2014
- November 2014
- October 2014
- September 2014
- August 2014
- July 2014
- June 2014
- May 2014
- April 2014
- March 2014
- February 2014
- January 2014
- December 2013
- November 2013
- October 2013
- September 2013
- August 2013
- July 2013
- June 2013
- May 2013
- April 2013
- March 2013
- February 2013
- January 2013
- December 2012
- November 2012
- October 2012
- September 2012
- August 2012
- July 2012
- June 2012
- May 2012
- April 2012
- March 2012
- February 2012
- January 2012
- December 2011
- November 2011
- October 2011
- September 2011
- August 2011
- July 2011
- June 2011
- May 2011
- April 2011
- March 2011
- February 2011
- January 2011
- December 2010
- November 2010
- October 2010
- September 2010
- August 2010
- July 2010
- June 2010
- May 2010
- April 2010
- March 2010
- February 2010
- January 2010
- December 2009
- November 2009
- October 2009
- September 2009
- August 2009
- July 2009
- June 2009
- May 2009
- April 2009
- March 2009
- February 2009
- January 2009
- December 2008
- November 2008
- October 2008
- September 2008
- August 2008
- July 2008
- June 2008
- May 2008
- April 2008
- March 2008
- February 2008
- January 2008
- December 2007
- November 2007
- October 2007
- September 2007
- August 2007
- July 2007
- June 2007
- May 2007
- April 2007
- March 2007
